15 Goal Attainment Scaling
- Log in [1] to post comments
WORK IN PROGRESS
We are improving this policy library. While work is underway, content of this chapter may not be the most current information available. Please contact rehabilitation@dva.gov.au [2] if you have any questions.

Overview of Goal Attainment Scaling
Goal Attainment Scaling is used within a DVA client’s Rehabilitation Plan to determine appropriate goals for the client, measure those goals against a standardised scale and, importantly, measure change and progress in the client’s functioning, employment, social and wellbeing outcomes.
Goal Attainment Scaling is a vital tool in DVA's rehabilitation program, as DVA clients often present with complex physical, psychological and social problems and may require a variety of rehabilitation goals.
Through a client-centred approach to goal development, DVA is able to improve rehabilitation outcomes within the framework of DVA’s whole-of-person model. It enables the comprehensive measurement of outcomes arising from a broad range of medical management, vocational and psychosocial goals, and highlights for the client the broad range of activities that make up a DVA Rehabilitation Plan.
15.1 Introduction to Goal Attainment Scaling
- Log in [3] to post comments
What is Goal Attainment Scaling?
DVA uses Goal Attainment Scaling to develop personal goals for clients during the development of their Rehabilitation Plan [4].
Providers work collaboratively with clients to tailor individual goals and to ensure they are appropriate and achievable. For each new goal, a scale is developed which describes specific outcomes.
Note: Goal Attainment Scaling is not required unless the client is participating in a whole‑of‑person Rehabilitation Plan which is being managed by a rehabilitation provider. This means that if a client is only being provided with specific services such as household services, attendant care services, assistance with motor vehicles, aids or appliances, then there is no requirement that the Goal Attainment Scaling process is used.
Examples
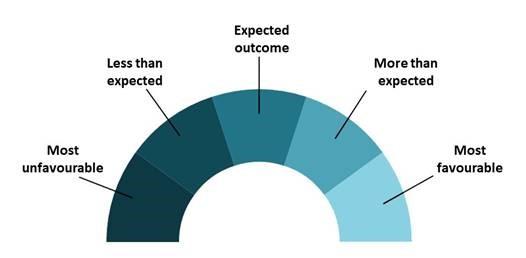
If a client sets a goal to "regain mobility outside of the home", the scale would identify the “expected” outcome for that individual, to be able to walk non-stop around their suburban block three times a week. A “more than expected” outcome would be to perform the walk five or six times a week. A “less than expected” outcome would be to only complete the walk once a week, or not at all.
Another example is shown in the diagram below with a goal to "secure and sustain employment".

The importance of scaling to DVA and its clients
Goal Attainment Scaling is aligned with DVA’s rehabilitation best practice philosophy [5] and emphasises the provision of individualised service and maximises client involvement in the development of plans and goals. Scaling formalises the collaborative element of the assessment and plan development process between provider and client.
Scaling improves DVA’s rehabilitation program by:
- ensuring all parties have the same understanding of the client’s rehabilitation goals via collaborative development;
- ensuring consistent expectations throughout the life of a Rehabilitation Plan by using well developed formal documentation; and
- assessing and reporting on improvements and changes to life satisfaction and wellbeing.
15.2 Roles and Responsibilities
Provider
The role of a provider is to assist clients in achieving desired outcomes through a whole-of-person rehabilitation program. Providers are responsible for assisting clients to develop high level goals [6] by identifying expected outcomes and then monitoring progress. The provider should:
- Make contact with the client within 7 days of receiving a referral from the Rehabilitation Delegate to undertake a rehabilitation assessment [7].
- If rehabilitation needs are identified, complete the client’s Rehabilitation Plan [4] within 21 days from initial contact regarding the rehabilitation assessment.
- In collaboration with the client, identify their rehabilitation needs by using a thorough assessment, develop rehabilitation goals, desired outcomes and activities.
- Assist the client to achieve their goals by working collaboratively with clients within the Goal Attainment Scaling (GAS) model.
- Ensure all relevant stakeholders have signed the Rehabilitation Plan before seeking final approval from the Rehabilitation Delegate.
- Regularly liaise with the Rehabilitation Delegate to update them on progress, in particular on specific issues or barriers.
- GAS outcomes must be recorded upon closure of the client’s rehabilitation plan. If the client is unable to advise their GAS outcome, providers should complete this information on the client’s behalf, to the best of their knowledge.
Rehabilitation Delegate
The role of the DVA Rehabilitation Delegate is to ensure clients achieve their goals by liaising with providers, and by monitoring client progress. Rehabilitation Delegates are responsible for reviewing rehabilitation assessment reports and approving an individual's rehabilitation plan, but are only required to do so once they are satisfied that the goals are achievable and will assist the client to achieve desired outcomes.
The Rehabilitation Delegate is responsible for transposing information from the documentation submitted by rehabilitation providers, into R&C ISH. This information includes goals, activities for each goal and GAS outcomes.
Client
DVA clients already have a number of rights and responsibilities relating to the development and undertaking of their rehabilitation plans. More information about these rights and responsibilities can be found in chapter 13 of this library [8] and in the relevant rights and obligations forms available through the DVA forms portal [9]. D1395 outlines a person's rights and obligations when participating in a return to work program. D1396 is to be used for clients who are participating in a non-return to work program.
Rehabilitation Goals are what the client wants to achieve through their rehabilitation plan. They will have a vocational, medical management or psychosocial focus. An example for each is provided below.
- Vocational goal – return to sustainable part-time work.
- Medical Management goal – identify appropriate medical professionals in my local area and start accessing treatment regularly.
- Psychosocial goal – to increase level of social activity and community participation.
A client may be working towards a mix of vocational, medical management and/or psychosocial goals concurrently, or may initially focus on achieving specific types of goals (e.g. medical management goals) before moving on to others. This will be determined by what is most appropriate for each client given their individual circumstances and needs.
15.3 DVA's Rehabilitation Process with Goal Attainment Scaling
- Log in [10] to post comments
This chapter provides guidance on how the DVA Rehabilitation Forms are completed using Goal Attainment Scaling.
15.3.2 Rehabilitation Assessment Report
- Log in [11] to post comments
Step 1. Enter client's name and DVA file number (not Defcare case ID) in the footer of the DVA Form D1334 Rehabilitation Assessment Report [12].
Step 2. Complete client details sections.
Step 3. Complete remainder of the Report.
Step 4. For all new rehabilitation referrals from 29 May 2017, upload the assessment report together with the rehabilitation plan and other relevant documentation to R&C ISH using the client's unique Transaction Reference Number. All existing rehabilitation cases that commenced prior to 29 May 2017 will require you to follow the current process of emailing rehabilitation related documentation to the client's Rehabilitation Coordinator.
15.3.3 Rehabilitation Plan
A rehabilitation plan is developed by the provider in conjunction with the client as a result of the rehabilitation assessment [7]. It may include medical management, psychosocial and/or return to work activities. The plan provides a structured series of individualised activities and goals.
The provider and client determine the rehabilitation goals (up to four) and set outcomes. Each goal has described five possible outcomes rated on a scale, ranging from the most unfavourable outcome through to the most favourable outcome. The middle point is identified as the “expected outcome”. The client and provider believe the client should be able to achieve at least the “expected outcome” by the end of the rehabilitation plan.
Goals vs Activities
Goals are what the client wants to achieve, or the desired outcome that they are working towards.
The rehabilitation activities are the things that the client will do to reach that outcome.
Goals should be specific, and as a general rule, multiple activities will be included to help the person to reach their goal. For example, the goal of ‘improvement to physical functioning’ could have the activities of ‘attend physiotherapy appointment 1 time per week and complete all exercises recommended by the therapist’, ‘walk around the block 4 times per week’ and ‘support from XX (eg. family member) to assist with developing a weekly routine’.
Completing the Rehabilitation Plan
When completing the DVA Form D1347 Rehabilitation Plan [13], the provider:
Step 1. Enters client’s name and the DVA file number (not the Defcare Case ID) in the footer of the document
Step 2. Completes client details section
Step 3. Defines rehabilitation goals, timeframes and categories
- 3.1 Provider and client to set relevant goals (up to four)* and timeframes
- 3.2 Notate the most applicable category for these specific goals: either medical management, vocational or psychosocial
Note: Providers should avoid setting goals and outcomes that could be too easily met or too difficult to achieve. Goals and expected outcomes should be described in such a way that the Coordinator is able to determine whether the goals are achievable.
Step 4. Define all rehabilitation outcomes
- 4.1 Describe the “expected outcome” and then describe the remaining rehabilitation outcomes.
Step 5. Define activities to achieve rehabilitation goal(s)
- 5.1 Discuss with the client, the activities to be undertaken to achieve the goal(s)
- 5.2 Record the general services that are required to achieve the goal (eg. relevant appointments, case management etc) and those that are more focused on what the client aims to do in order to achieve the specific outcomes (eg. doing exercise or a social activity)
Step 6. Specify parties involved for the activities and dates associated with each activity
- 6.1 Specify the parties involved e.g. the client, provider, employer, medical professional, etc
- 6.2 Specify the start and end dates for the activities (do not have to reflect the same start or end dates as the overarching Plan but must not go outside the start and end dates of the Plan)
Step 7. Indicate importance and challenges in achieving each goal
- 7.1 Mark the appropriate boxes to indicate the level of importance and challenge (a little, moderately or very) the client identifies for each goal
Step 8. Complete agreement section ('Sign-Off and Distribution')
- 8.1 When goals, outcomes and activities have been agreed between the provider and client, the Plan is signed by client and provider
Step 9. Indicate costs involved with activities outlined in the Plan
- 9.1 Identify all relevant goals for each activity
- 9.2 Indicate the costs involved in terms of provider costs, third party costs and the total costs for each activity identified in the Plan
Step 10. Processing Rehabilitation plan documentation
- 10.1 Upload the rehabilitation plan together with the assessment report and any relevant documentation to R&C ISH using the client's unique Transaction Reference Number.
- 10.2 Once the Rehabilitation Coordinator has approved the plan, it can commence.
- 10.3 Rehabilitation Coordinators are responsible for transposing information from the rehabilitation plan submitted by rehabilitation providers, into R&C ISH. This information includes goals and activities for each goal.
IMPORTANT: The rehabilitation provider must ensure that no treatment costs are included on a medical management Rehabilitation Plan. Treatment costs are covered by the normal medical payment arrangements, usually through the DVA Health Card system.
* Note: It is considered, as a general rule, that too many goals may have a negative impact on the client as they may be trying to achieve too much in a short space of time. However, setting more than four goals might be appropriate, in some circumstances, if the provider and client consider it could be beneficial for the client and they are highly motivated. It is important that the provider and client are both confident that the client could be realistically expected to achieve more than four goals, before these are included on the rehabilitation plan.
15.3.4 Rehabilitation Plan Amendment
A Rehabilitation Plan Amendment is completed:
- *when any changes to goals [14] and/or the short or long term activities are required;
- if the timeframes to complete activities of the plan need to be adjusted (this includes an extension to the Plan itself);
- *if additional rehabilitation activities need to be included; or
- where the approved funding for the plan activities requires a minor amendment.
NOTE: A Rehabilitation Plan Amendment is not used when the overall focus of the client's rehabilitation program changes, for example, where a client moves from a non-return to work program to a return to work program, or vice versa. Where this occurs, the original program should be varied by the creation of a new Plan. DVA Rehabilitation Coordinators must issue a determination letter whenever a rehabilitation program is varied. More information about this can be found in section 3.8.4 of this Guide [15].
* It is not necessary to make an amendment to a Plan if the client is unable to undertake all planned future activities related to an existing goal in the current Plan. In such cases, before the Plan is discussed with the client, it should be considered whether the client’s primary care provider (GP, specialist) should be engaged to help the client to manage any particular health issue which may be preventing the client from currently undertaking that activity or achieving their rehabilitation goal.
Goals vs Activities
Goals are what the client wants to achieve, or the desired outcome that they are working towards.
The rehabilitation activities are the things that the client will do to reach that outcome.
Goals should be specific, and as a general rule, multiple activities will be included to help the person to reach their goal. For example, the goal of ‘improvement to physical functioning’ could have the activities of ‘attend physiotherapy appointment 1 time per week and complete all exercises recommended by the therapist’, ‘walk around the block 4 times per week’ and ‘support from XX (e.g. family member) to assist with developing a weekly routine’.
New or Amended Goal
When completing the DVA Form D1336 Rehabilitation Plan Amendment [13], the provider:
Step 1. Enters client’s name and the DVA file number (not the Defcare Case ID) in the footer of the document
Step 2. Completes client details section
Step 3. Defines rehabilitation goals, timeframes and categories
- 3.1 Provider and client to set relevant goals (up to four) and timeframes
- 3.2 Notate the most applicable category for these specific goals: either medical management, vocational or psychosocial
Note: Providers should avoid setting goals and outcomes that could be too easily met or too difficult to achieve. Goals and expected outcomes should be described in such a way that the Coordinator is able to determine whether the goals are achievable.
Step 4. Define all rehabilitation outcomes
- 4.1 Describe the “expected outcome” and then describe the remaining rehabilitation outcomes.
Step 5. Define activities to achieve rehabilitation goal(s)
- 5.1 Discuss with the client, the activities to be undertaken to achieve the goal(s)
- 5.2 Record the general services that are required to achieve the goal (eg. relevant appointments, case management etc) and those that are more focused on what the client aims to do in order to achieve the specific outcomes (eg. doing exercise or a social activity)
Step 6. Specify parties involved for the activities and dates associated with each activity
- 6.1 Specify the parties involved e.g. the client, provider, employer, medical professional, etc
- 6.2 Specify the start and end dates for the activities (do not have to reflect the same start or end dates as the overarching Plan but must not go outside the start and end dates of the Plan)
Step 7. Indicate importance and challenges in achieving each goal
- 7.1 Mark the appropriate boxes to indicate the level of importance and challenge (a little, moderately or very) the client identifies for each goal
Step 8. Complete agreement section ('Sign-Off and Distribution')
- 8.1 When goals, outcomes and activities have been agreed between the provider and client, the Plan Amendment is signed by client and provider
Step 9. Indicate costs involved with activities outlined in the Plan Amendment
- 9.1 Identify all relevant goals for each activity
- 9.2 Indicate the costs involved in terms of provider costs, third party costs and the total costs for each activity identified in the Plan
Step 10: Processing rehabilitation plan amendment documentation
- 10.1 Upload the rehabilitation plan amendment and any other relevant documentation to R&C ISH using the client's unique Transaction Reference Number (TRN).
- 10.2 Once the Coordinator has approved the Plan Amendment, it can commence.
- 10.3 Rehabilitation Coordinators are responsible for transposing information from the rehabilitation plan amendment submitted by rehabilitation providers, into R&C ISH. This information includes goals and activities for each goal.
IMPORTANT: The provider must ensure that no treatment costs are included on a medical management Rehabilitation Plan. Treatment costs are covered by the normal medical payment arrangements, usually through the DVA Health Card system.
# It is considered that, as a general rule, too many goals may have a negative impact on the client as they may be trying to achieve too much in a short space of time. However, setting more than four goals might be appropriate in some circumstances if the provider and client consider it could be beneficial for the client and they are highly motivated. It is important that the provider and client are both confident that the client could be realistically expected to achieve more than four goals, before these are included on the Rehabilitation Plan.
Change of Outcome(s)
If a change to any outcome is required, an amendment may be undertaken. This may occur if there are exceptional and unanticipated circumstances that have arisen since plan development. This ensures all clients attain their expected outcomes.
Change of Activities or Timeframes Where Goals Have Not Changed
If a change of timeframes is required, but the goal(s) remains the same, the activities associated with the goal may be revised, or new activities added for that goal. When amending or adding new activities, the provider must indicate the parties involved, dates for each new activity, and any costs associated with the activities .
If the only change is to extend the time of the plan, to enable extra time for rehabilitation activities to be completed, the GAS information is not required as it is already included in the Rehabilitation Plan. Information should be provided in the amendment about why the extra time is required.
Rehabilitation Goals are what the client wants to achieve through their rehabilitation plan. They will have a vocational, medical management or psychosocial focus. An example for each is provided below.
- Vocational goal – return to sustainable part-time work.
- Medical Management goal – identify appropriate medical professionals in my local area and start accessing treatment regularly.
- Psychosocial goal – to increase level of social activity and community participation.
A client may be working towards a mix of vocational, medical management and/or psychosocial goals concurrently, or may initially focus on achieving specific types of goals (e.g. medical management goals) before moving on to others. This will be determined by what is most appropriate for each client given their individual circumstances and needs.
15.3.5 Progress Reports
Goals vs Activities
Goals are what the client wants to achieve, or the desired outcome that they are working towards.
The rehabilitation activities are the things that the client will do to reach that outcome.
Goals should be specific, and as a general rule, multiple activities will be included to help the person to reach their goal. For example, the goal of ‘improvement to physical functioning’ could have the activities of ‘attend physiotherapy appointment 1 time per week and complete all exercises recommended by the therapist’, ‘walk around the block 4 times per week’ and ‘support from XX (eg. family member) to assist with developing a weekly routine’.
Progress Report
For the DVA Form D1330 Rehabilitation Progress Report [13], the provider will:
Step 1. Enter the client’s name and DVA file number (not Defcare Case ID) in the footer of the document.
Step 2. Complete the client details section
Step 3. Document the identified activities for each goal.
Step 4. Provide a summary of the Progress Report.
Step 5. Sign the Progress Report. Upload the Progress Report and any other relevant documentation to R&C ISH using the client's unique Transaction Reference Number (TRN). Rehabilitation Coordinators are not required to sign the Progress Report.
Step 6. Rehabilitation Coordinators are responsible for transposing information from the documentation submitted by the rehabilitation providers, into R&C ISH. This information includes goals and activities for each goal.
15.3.6 Rehabilitation Closure Report
For the DVA Form D1335 Rehabilitation Closure Report [13], the provider will:
Step 1. Complete client’s name and DVA File Number (not Defcare Case ID) in the footer of the document.
Step 2. Complete client and plan details sections.
Step 3. Determine Goal Attainment Scaling outcomes and activities
- 3.1 Discuss with the client their progress in relation to each goal [14] described in the plan. If a client is uncontactable for any reason at closure, the provider completes the next step to the best of their knowledge.
- 3.2 Based on the criteria describing each outcome, determine whether the client has achieved the ‘expected outcome’, ‘more than expected’ outcome or ‘most favourable’ outcome. Conversely, if the client has achieved ‘less than expected’ outcome or ‘most unfavourable’ outcome.
- 3.3 Report on activities, including status.
Step 4. Complete agreement section (Sign-Off and Distribution of Closure Report)
Step 5. Indicate costs incurred with activities outlined in the final Rehabilitation Plan
- 5.1 Provider indicates the costs involved in terms of total provider costs, third party costs and the total costs involved with the final plan.
Step 6. Upload the closure report and any other relevant documentation into R&C ISH using the client's unique Transaction Reference Number (TRN).
Step 7. Rehabilitation Coordinators are responsible for transposing information from the documentation submitted by rehabilitation providers, into R&C ISH. This information includes goals and activities for each goal.
Rehabilitation Goals are what the client wants to achieve through their rehabilitation plan. They will have a vocational, medical management or psychosocial focus. An example for each is provided below.
- Vocational goal – return to sustainable part-time work.
- Medical Management goal – identify appropriate medical professionals in my local area and start accessing treatment regularly.
- Psychosocial goal – to increase level of social activity and community participation.
A client may be working towards a mix of vocational, medical management and/or psychosocial goals concurrently, or may initially focus on achieving specific types of goals (e.g. medical management goals) before moving on to others. This will be determined by what is most appropriate for each client given their individual circumstances and needs.
15.4 Outcome Reporting
Goal Attainment Scaling (GAS) outcome reporting provides DVA with a link between the whole-of-person model of rehabilitation and the measurement of whole of-person outcomes. Reporting data obtained by the GAS process assists DVA to understand the level of success or otherwise for clients receiving rehabilitation services.
The increased detail that GAS generates for reporting purposes is crucial in assisting DVA to better understand clients’ needs and ensure the services delivered best support those in need. With GAS, DVA will be able to clearly define and report on the broad range of client services and support and better address complex and whole‑of‑person needs. Reporting options include:
- medical management, vocational and psychosocial outcomes achieved through a whole‑of‑person program;
- average GAS outcomes;
- individual GAS outcomes;
- achievements in positive outcomes for clients or where additional/further support is required;
- the number of plans involving more than one type of rehabilitation intervention, i.e. vocational, psychosocial or medical management; and
- information on provider performance results.
15.5 Case Example for Goal Attainment Scaling
Debra is a 28 year old former Reservist Army Corporal (Combat Medical Assistant). Her main role in the reserve force was medical records manager. She works full time as a paramedic and is highly skilled in administration.
Debra does not have a partner and has one child who is 7 years old. As a paramedic officer, Debra’s civilian role is physically and mentally demanding as she is required to undertake a range of activities varying from patient care and transport to emergency response and assistance.
Debra was medically discharged in December 2009 after which DVA accepted liability for an injury to her right knee. Debra has been transferred to an administrative role in her civilian workplace as her knee injury resolves. She is not able to work as a paramedic until pain, swelling and mobility issues are addressed.
Following the acceptance of liability by DVA, a needs assessment was undertaken which resulted in Debra being referred to a local rehabilitation provider and Occupational Therapist (OT).
The provider assessed Debra and identified areas where the client was having difficulties with her health and wellbeing. The assessment outlined her main symptoms as:
- chronic pain and swelling, as a result of severe ligament and patella damage to her right knee;
- severe mobility issues and minimal weight bearing capacity;
- difficulties with accessing medical treatment to address knee injury and no clear treatment plan;
- difficulties with managing pain caused by knee injury;
- diagnosed depression – Debra is having difficulties in coping with her discharge from the reserve force, inability to fulfil her paramedic role and managing her household responsibilities and caring for her child.
The following Rehabilitation Plan [4] was developed to address her needs:
- a medical management Rehabilitation Plan to help her to manage her physical and mental health and treatment needs and coordinate her medical appointments;
- a psychosocial Rehabilitation Plan including attendance at a pain management program;
- provision of a walking aid and simple home modifications (ramps) through the Rehabilitation Appliances Program;
- household services to assist with management of house cleaning and washing prior to surgery, and additional tasks for a period while recovering from surgery; and
- attendant care services to assist with personal care needs post surgery.
Debra and the provider developed the following goals [6] under a medical management and psychosocial Rehabilitation Plan.
| Level of expected outcome | Goal 1: Access treatment for knee condition and be following recovery plan | Goal 2: Improve mood/mental health | Goal 3: Improve management of pain |
|---|---|---|---|
Most favourable outcome | Knee replacement surgery has occurred within three months and knee is progressing better than expected so there is no pain or swelling three months post surgery as a result of following recovery plan | Has accessed treatment for depression and managing symptoms effectively 50% of the time within three months | Has participated in pain management program and is managing pain symptoms effectively 50% of the time within three months |
More than expected outcome | Knee replacement surgery has occurred within three months and knee is progressing as expected so there is little pain or swelling three months post-surgery as a result of following recovery plan | Has accessed treatment for depression and managing symptoms effectively 25% of the time within three months | Has participated in pain management program and is managing pain symptoms effectively 25% of the time within three months |
Expected outcome | Knee replacement surgery has occurred within three months and there is a recovery plan in place | Has accessed treatment for depression and is learning strategies to manage symptoms within three months | Is participating in pain management program and is learning strategies to manage pain within three months |
Less than expected outcome | Knee replacement surgery did not occur within three months, but has seen surgeon and date is set. There is an active management plan in place for managing injury while awaiting surgery | Is yet to access treatment for depression and there is no change in depression symptoms | Is yet to participate in pain management program and there is no change in ability to manage pain |
Most unfavourable outcome | Knee replacement surgery did not occur within three months, has had no contact with surgeon or other health professional and no active management plan in place | Is yet to access treatment for depression and symptoms have worsened | Is yet to participate in pain management program and pain has worsened |
At the Progress Report [16] stage, Debra and her provider reviewed the original assessment and identified that Debra is recovering well from knee surgery with less pain and greater mobility. Debra still requires household services, but this will be reviewed as her recovery continues. Her depression treatment and support is also progressing well and Debra is pleased to be able to return to her role as a paramedic officer. Debra also received workplace modifications, as recommended by the OT.
| Level of expected outcome | Goal 1: Access treatment for knee condition and follow recovery plan - 1 Month Follow Up | Goal 2: Improve mood/mental health - 3 Month Follow Up | Goal 3: Improve management of pain - 3 Month Follow Up |
|---|---|---|---|
Most favourable outcome | |||
More than expected outcome | X | X | |
Expected outcome | X | ||
Less than expected outcome | |||
Most unfavourable outcome |
Rehabilitation Goals are what the client wants to achieve through their rehabilitation plan. They will have a vocational, medical management or psychosocial focus. An example for each is provided below.
- Vocational goal – return to sustainable part-time work.
- Medical Management goal – identify appropriate medical professionals in my local area and start accessing treatment regularly.
- Psychosocial goal – to increase level of social activity and community participation.
A client may be working towards a mix of vocational, medical management and/or psychosocial goals concurrently, or may initially focus on achieving specific types of goals (e.g. medical management goals) before moving on to others. This will be determined by what is most appropriate for each client given their individual circumstances and needs.
Links
[1] https://clik.dva.gov.au/user/login?destination=comment/reply/79519%23comment-form
[2] mailto:rehabilitation@dva.gov.au
[3] https://clik.dva.gov.au/user/login?destination=comment/reply/79523%23comment-form
[4] https://clik.dva.gov.au/node/79528
[5] https://clik.dva.gov.au/rehabilitation-policy-library/1-introduction-rehabilitation/13-dva-rehabilitation-framework
[6] https://clik.dva.gov.au/%23
[7] https://clik.dva.gov.au/rehabilitation-policy-library/15-goal-attainment-scaling/153-dvas-rehabilitation-process-goal-attainment-scaling/1532-rehabilitation-assessment-report
[8] https://clik.dva.gov.au/rehabilitation-policy-library/13-rights-and-obligations
[9] https://www.dva.gov.au/about-us/forms
[10] https://clik.dva.gov.au/user/login?destination=comment/reply/79525%23comment-form
[11] https://clik.dva.gov.au/user/login?destination=comment/reply/79527%23comment-form
[12] https://www.dva.gov.au/about-us/dva-forms/rehabilitation-assessment-report
[13] https://www.dva.gov.au/get-support/find-forms
[14] https://clik.dva.gov.au/rehabilitation-policy-library/15-goal-attainment-scaling/153-dvas-rehabilitation-process-goal-attainment-scaling/1533-rehabilitation-plan
[15] https://clik.dva.gov.au/rehabilitation-policy-library/3-rehabilitation-process/38-dva-rehabilitation-reporting-documents/384-changes-rehabilitation-plan
[16] https://clik.dva.gov.au/node/79531